
In state after state, the arrival of adult-use cannabis set off a slow, measurable erosion of the medical tier. Not a collapse — a steady bleed. Michigan lost 79 percent of its medical dispensary licenses from peak. New Mexico shed a fifth of its registered patients in twelve months. The medical tier was losing share. The cannabis market was not.
Then the federal government rescheduled cannabis. Medical, now Schedule III, is no longer subject to IRC Section 280E — the provision that has cost operators billions in disallowed deductions since the 1980s. Adult-use remains Schedule I. The same product, sold from the same building, now carries a different federal tax burden depending on which side of the dual-license ledger it lands on. That is a structural advantage, and it may be the first real one medical has had in years.

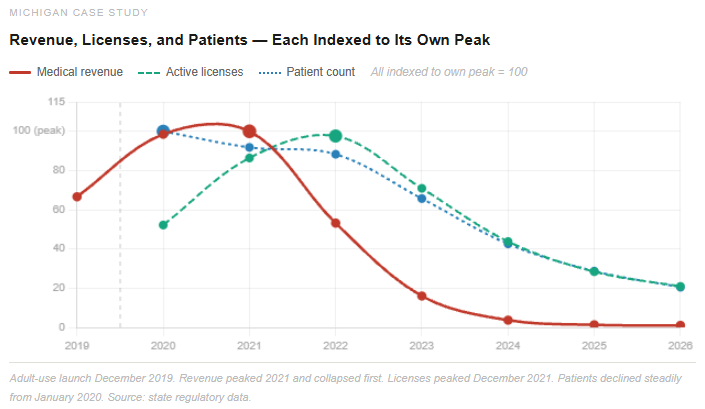
Across four datasets and thirty-two reporting states, one finding keeps surfacing: revenue is the leading indicator of medical program health, patient counts are the lagging one, and license counts fall somewhere in between. Sales crack first. Patient rolls thin last. Michigan’s revenue peaked in 2021. Its patient count didn’t look alarming for another two years. By then the revenue signal had been flashing red for years.

The Michigan data makes the point starkly. A Michigan medical card is valid for two years — yet enrollment dropped within months of adult-use launching in December 2019. Patients didn’t wait for renewal. They walked away from credentials they’d already paid for, mid-cycle. The medical card is not an identity or a loyalty — it is a procurement credential, held when it represents the easiest path to the product and abandoned when something easier appears. The moment adult-use shelves opened, the card’s value proposition collapsed faster than the two-year renewal cycle would predict.
Rescheduling changes that calculus. If medical operators pass the 280E savings through to price, patients currently renewing out of habit have a concrete reason to stay. Adults buying adult-use who have never held a card have a reason to get one. Pennsylvania — $1.8 billion in medical revenue, 439,000 patients, growing every year with no adult-use competitor — is the ceiling estimate for what an undisrupted medical program produces. Rescheduling doesn’t recreate Pennsylvania’s conditions, but it shifts the economics in that direction.
Two states define the range of what comes next. Oklahoma implemented a license moratorium after its medical market became the most overcrowded in the country; licenses are falling by attrition while revenue and patients still run. It may become the clearest test of what a rationalized medical market looks like when the tax environment works in its favor. Florida — 918,000 patients, unlimited stores per license, infrastructure already built at scale — is the largest untransitioned market in the country. When adult-use eventually clears there, all three signals will move at once. The data will be unlike anything the industry has seen from a prior transition.
Medical cannabis didn’t fail. Something faster appeared beside it. Rescheduling changes the economics without changing that underlying logic — it gives operators a reason to invest in the medical channel at a moment when most had stopped. Whether they act on it is what the next several years of sales, enrollment, and pricing data will answer.
For a more in-depth leading state analysis go to https://hubs.la/Q04j_XfC0
